
Growing and converging evidence suggests that the motor system becomes integrated with the complex processing of nociceptive signals. In patients with amputated limbs, part of the primary motor cortex becomes redundant for its prior tasks, while also being deprived of the sensory feedback. When a critical role of the motor cortex, that of suppressing excessive sensory input into the thalamus and inducing descending pain modulation, is compromised, spontaneous pain may result.
Finnish rTMS patient cases
Hear first hand from a patient in the Helsinki University Hospital & Orton pain treatment program, how navigated rTMS changed his live (subtitles are available in English) and see two more case examples from Turku University Hospital in Finland.
rTMS offers a truly significant analgesic effect
In patients with neuropathic pain, evidence-based guidelines on the therapeutic use of repetitive transcranial magnetic stimulation1 make a Level A recommendation for the truly significant analgesic effect of high-frequency rTMS targeted at the motor cortex, contralaterally to the pain side. Tolerance of rTMS is rated as excellent, even in patients with chronic refractory pain.
rTMS has shown better efficacy in patients with neuropathic pain of cortical or peripheral origin than in patients with lesions affecting the brainstem or the spinal cord.
1. Lefaucheur, J.-P. et al. Evidence-based guidelines on the therapeutic use of repetitive transcranial magnetic stimulation (rTMS): An update (2014–2018). Clinical Neurophysiology 131, 474–528 (2020).
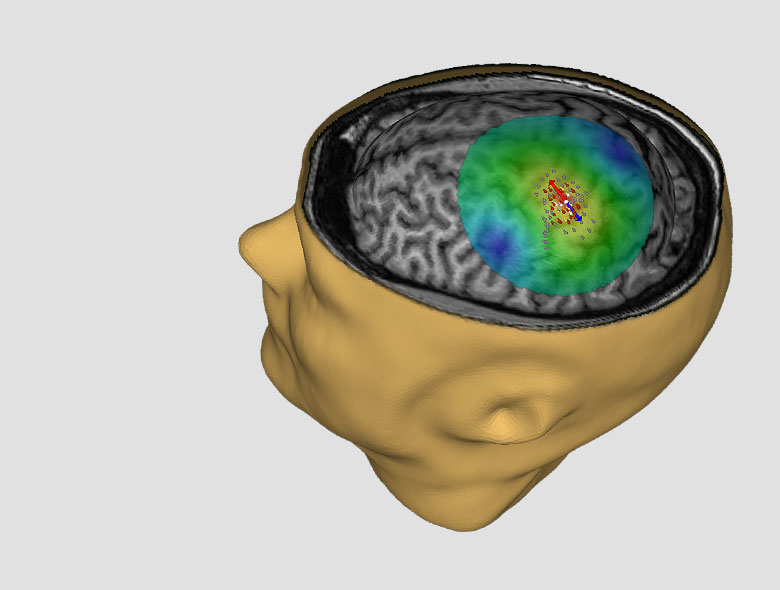
Target site selection
Experts agree that image-guidance of the therapy — the NBS 6 with SmartFocus® nTMS — is required, since determining the exact stimulation site within the motor cortex is critical for obtaining the optimal therapeutic response. Cortical reorganization can add an additional challenge in selecting a site for targeting the stimulation and numerous studies have shown evidence of more pronounced analgesic effects when the region adjacent to the painful region is targeted with rTMS.
In chronic pain there is significant cortical reorganization within the primary motor cortex and the corticomotor maps are in a state of flux. rTMS treatment can normalize the representation area of the primary motor cortex and have a therapeutic effect—patients who do not respond to rTMS therapy have not shown normalization in the motor cortex.
Stimulation parameters and durability
The analgesic effects of rTMS depend on the frequency of stimulation. When targeted to the motor cortex contralateral to the painful side at frequencies of 5 Hz, or higher, rTMS may provide pain relief. The analgesic effects of rTMS are related to the excitation of neural circuits lying in the superficial layers of the cortex, tangential to the surface of the precentral gyrus.
High frequency rTMS increases cortical excitability beyond the time of stimulation. The maximal analgesic effect of a single session of rTMS occurs after 2–3 days and may extend for up to one week. In fibromyalgia, it has been shown that pain control can be maintained for up to six months by monthly rTMS treatments, following an induction phase of daily 20-min rTMS sessions for 5 days.
Nexstim Protocol (CE mark)
In patients suffering from unilateral chronic neuropathic pain, the motor representation area corresponding to the pain location on the hemisphere contralateral to pain is enlarged2. With Nexstim the specific cortical targets for rTMS delivery are obtained by bilateral motor cortex mapping of both hemispheres and comparing the motor representation areas to each other. The primary therapy target is chosen as the hotspot of muscle representation area of the muscle corresponding to the location of pain (for hand pain – First Dorsal Interosseus muscle, for leg pain – m.Tibialis Anterior, for facial pain – m.Orbicularis Oris) that also resides within the mirror image of the same motor representation area on the unlesioned hemisphere. After the target is localized, the Nexstim System is used to determine the patient’s individual MT of the target location. With the stimulator output set to up to 100% intensity of individual MT, the rTMS therapy (10 Hz, 20 trains of 100 pulses, total of 2000 pulses) is then started. If, after 2-3 treatment sessions no response is obtained, stimulation of a second therapy target - the motor cortex hotspot of the muscle representation area contralateral to the pain that is outside the corresponding representation area of the same muscle on the unaffected hemisphere may result in clinical benefit (see below).
2. Nurmikko, T. et al. Motor cortex reorganization and repetitive transcranial magnetic stimulation for pain: a methodological study. Neuromodulation 19, 669–678 (2016).
Pre-surgical rTMS therapy in MCS implantation
Although epidural MCS can be an effective method to treat drug-resistant neuropathic pain, the procedure is invasive and there are no reliable preoperative criteria to predict outcome.
As a non-invasive technology, rTMS can play a role in identifying responders to MCS pre-surgically. Patients who respond to rTMS respond to MCS with an extremely high positive predictive value, although rTMS has a low predictive value to rule patients out from surgery. A positive response to rTMS therapy can help patients accept epidural implantation.
The validation of a cortical target by preoperative rTMS helps neurosurgeons plan and optimize epidural electrode placement in MCS implantation.
Interested in a live demo of nTMS?
Our team of physicians, researchers, and engineers is prepared to answer your questions. If you would like to learn more or set up a virtual demonstration for your team, please contact us!
Yes, I would like to know more
Patient Safety
SAFETY
NBS 6 THERAPY SHOULD NOT BE GIVEN TO
- Patients with non-removable conductive, ferromagnetic, or other magnetic-sensitive metal anywhere in the head or within 30 cm (12 in) of the stimulation coil. Examples include cochlear implants, implanted electrodes or stimulators, aneurysm clips or coils, stents, bullet fragments, ocular implants, and stents.
- Patients who have an active or inactive implanted device (including device leads), including deep brain stimulators, cochlear implants, cardiac pacemakers, and vagus nerve stimulators. Contraindicated use could result in serious injury or death.
- Patients with increased intracranial pressure or patients with intracardiac lines, intravenous pumps, or dose calculators.
Failure to follow these restrictions could result in serious injury or death.
RISKS AND SIDE EFFECTS
Seizures (Convulsions): Cortical magnetic stimulation runs the risk of inducing seizures; although they are rare.
The most common side effects reported during clinical studies (Lefaucheur et al., Nurmikko et al.) are: mild headache (25% of the TMS treatment group), sleepiness (38 %), and dizziness (15 %).
No severe adverse events were reported. Specifically, no seizures occurred.
In some patients with chronic neuropathic pain, the pain may transiently worsen after rTMS stimulation. The increase in pain sensation may last up to 1-2 days.
No adverse effects on hearing have occurred when ear protection has been properly worn.
No effects on cognitive function has been reported.
Clinical studies have reported no deaths in rTMS therapy. (Nurmikko et al.)
References
1. Lefaucheur, J.-P. et al. Evidence-based guidelines on the therapeutic use of repetitive transcranial magnetic stimulation (rTMS): An update (2014–2018). Clinical Neurophysiology 131, 474–528 (2020).
2. Nurmikko, T. et al. Motor cortex reorganization and repetitive transcranial magnetic stimulation for pain: a methodological study. Neuromodulation 19, 669–678 (2016).
Others:
Ahdab, R. & Lefaucheur, J.-P. 2nd International Symposium on Navigated Brain Stimulation in Neurosurgery, Charité – Universitätsmedizin Berlin, 34–36 (2011).
Mylius, V. & Lefaucheur, J.-P. 3rd International Symposium on Navigated Brain Stimulation in Neurosurgery, Charité – Universitätsmedizin Berlin, 27–29 (2012).
Nurmikko, T. J. & Sacco, P. 3rd International Symposium on Navigated Brain Stimulation in Neurosurgery, Charité – Universitätsmedizin Berlin, 23–26 (2012).
Nurmikko, T. J. & Sacco, P. 5th International Symposium on Navigated Brain Stimulation in Neurosurgery, Charité – Universitätsmedizin Berlin, 32–36 (2014).
Regulatory Approval
Nexstim is a medical device manufacturer. Nexstim NBS 6 is an FDA-cleared and CE-marked medical device (notified body number: 0537). For more information on individual regional clearances, please refer to the table, intended purpose and indications for use descriptions below:
| Clinical Application | European Union (CE mark) | United States (FDA) |
| Pre‑procedural Mapping | CE‑marked | FDA cleared |
| Post‑operative Motor Rehabilitation | CE‑marked | Investigational use only |
| Major Depressive Disorder (Adults) | CE‑marked | FDA cleared |
| Major Depressive Disorder (Adolescents) | Not CE‑marked | FDA cleared |
| Obsessive‑Compulsive Disorder | Not CE‑marked | FDA cleared |
| Chronic Neuropathic Pain | CE‑marked | Investigational use only |
Indications for use & Intended purpose
Pre-procedural mapping (CE mark, FDA clearance, for information on other regional clearances contact Nexstim):
Intended purpose: NBS 6 is intended to be used for localization and assessment of the motor cortex and motor tract integrity for pre-procedural planning purposes. NBS 6 is intended to be used for localization and assessment of cortical areas of speech function for pre-procedural planning purposes.
Indications for use: NBS 6 is indicated for noninvasive mapping of the primary motor cortex of the brain to its cortical gyrus. NBS 6 provides information that may be used in the assessment of the primary motor cortex for pre-procedural planning. NBS 6 is indicated for noninvasive localizations of cortical areas that do not contain essential speech function. NBS 6 provides information that may be used in pre-surgical planning in patients undergoing brain surgery. Intraoperatively, the localization information provided by NBS 6 is intended to be verified by direct cortical stimulation. NBS 6 is not intended to be used during a surgical procedure. NBS 6 is intended to be used by trained clinical professionals.
Post-operative Rehabilitation (CE mark, for information on other regional clearances contact Nexstim):
Intended purpose: NBS 6 is intended to be used for the treatment of surgically induced new or worsening post-operative motor deficits of the upper limb as an adjunct therapy for motor rehabilitation in adult patients having undergone brain tumor surgery. NBS 6 is intended to be used by trained clinical professionals.
Nexstim NBS 6 is not cleared by the FDA for commercial use of post-operative rehabilitation in the United States, for investigational use only.
Chronic Neuropathic Pain (CE mark, for information on other regional clearances contact Nexstim):
Intended purpose: In adult patients suffering from chronic unilateral neuropathic pain, NBS 6 is intended to provide electric field navigated noninvasive repetitive TMS stimulation as therapy to alleviate pain. NBS 6 is intended to be used by trained clinical professionals.
Indications for use: NBS 6 is indicated for MRI-guided and electric field (or E-field) navigated, noninvasive repetitive TMS stimulation (rTMS) of the motor cortex as therapy to alleviate chronic unilateral neuropathic pain in adult patients. Nexstim NBS 6 is intended to be used by trained clinical professionals.
Nexstim NBS 6 is not cleared by the FDA for commercial use of the treatment of chronic pain in the United States, for investigational use only.
Major Depressive Disorder (CE mark, FDA clearance, for information on other regional clearances contact Nexstim):
Intended purpose: NBS 6 is intended to be used for treatment of major depressive disorder (MDD) by targeting and delivering noninvasive repetitive TMS stimulation to the patient's dorsolateral prefrontal cortex.
Indications for use: NBS 6 is indicated for the treatment of Major Depressive Disorder in adult patients who have failed to achieve satisfactory improvement from prior antidepressant medication in the current episode. NBS 6 is intended to be use by trained clinical professionals.
Adolescent Major Depressive Disorder (FDA clearance, for information on other regional clearances contact Nexstim):
Indications for use: NBS 6 is indicated as an adjunct for the treatment of MDD in adolescent patients (age 15-21).
Obsessive-Compulsive Disorder (FDA clearance, for information on other regional clearances contact Nexstim):
Indications for use: NBS 6 is indicated as an adjunct for the treatment of adult patients suffering from obsessive-compulsive disorder (OCD).